
[ad_1]
MRSA infections had dropped for years, however the COVID-19 pandemic erased years of progress. In the course of the pandemic, some infections attributable to MRSA rose 41%, in keeping with the Society for Healthcare Epidemiology of America.
Provided that MRSA is alleged to unfold by contact (fomite transmission), hand-washing — Hospital An infection Management loves them their handwashing — is one acceptable treatment, together with disinfecting surfaces. From CDC’s web page on “Cleansing & Disinfection” (final reviewed February 27, 2019):
")
However what if MRSA can be airborne?
Is MRSA Airborne?
Here’s a checklist of research suggesting that it’s (with, sadly, some hyperlink rot, although typically looking on the title does the trick). For instance, Journal of Hospital An infection, “Discount in MRSA environmental contamination with a conveyable HEPA-filtration unit” (2006):
The purpose of this research was to judge the effectiveness of a conveyable high-efficiency particulate air (HEPA)-filtration unit (IQAir Cleanroom H13, Incen AG, Goldach, Switzerland) at lowering MRSA environmental floor contamination inside a medical setting. The MRSA contamination charge on horizontal surfaces was assessed with agar settle plates in ward side-rooms of three sufferers who had been heavy MRSA dispersers. … With out air filtration, between 80% and 100% of settle plates had been optimistic for MRSA… Air filtration at a charge of 140 m(3)/h (one affected person) and 235 m(3)/h (two sufferers), resulted in a extremely vital lower in contamination charges in contrast with no air filtration…. In conclusion, this moveable HEPA-filtration unit can considerably scale back MRSA environmental contamination inside affected person isolation rooms, and this will likely show to be a helpful addition to current MRSA an infection management measures.
If MRSA weren’t airborne, HEPA filters would hardly scale back it, amiright or amiright? Right here’s one other one, from JAMA, “Significance of Airborne Transmission of Methicillin-Resistant Staphylococcus aureus in an Otolaryngology–Head and Neck Surgical procedure Unit” (2001):
The MRSA samples had been collected from the air in single-patient rooms throughout each a interval of relaxation and when bedsheets had been being modified. Isolates of MRSA had been detected in all levels (from stage 1 [>7 µm] to stage 6 [0.65-1.1 µm]). About 20% of the MRSA particles had been inside a respirable vary of lower than 4 µm. Methicillin-resistant S aureus was additionally remoted from inanimate environments, resembling sinks, flooring, and bedsheets, within the rooms of the sufferers with MRSA infections in addition to from the sufferers’ fingers. An epidemiological research demonstrated that medical isolates of MRSA in our ward had been of 1 origin and that the isolates from the air and from inanimate environments had been similar to the MRSA strains that brought about an infection or colonization within the inpatients.
Methicillin-resistant S aureus was recirculated among the many sufferers, the air, and the inamimate environments, particularly when there was motion within the rooms. Airborne MRSA might play a job in MRSA colonization within the nasal cavity or in respiratory tract MRSA infections. Measures must be taken to forestall the unfold of airborne MRSA to manage nosocomial MRSA an infection in hospitals.
And another, from Anesthesia and Intensive Care (PDF), “The Correlation Between Airborne Methicillin-resistant Staphylococcus aureus with the Presence of MRSA Colonized Sufferers in a Basic Intensive Care Unit” (2004):
Air sampling straight onto a methicillin-resistant Staphylococcus aureus (MRSA) selective agar was carried out at six places 3 times weekly over a interval of 32 weeks in a brand new, initially MRSA-free Intensive Care Unit to look at if MRSA is current in air pattern cultures and, in that case, whether or not it’s affected by the variety of MRSA colonized sufferers current. A complete of 480 air samples had been collected on 80 days. A complete of 39/480 (8.1%) samples had been discovered to be MRSA optimistic of which 24/160 (15%) optimistic air samples had been from the only rooms, the place MRSA colonised sufferers had been remoted, and 15/320 (4.7%) had been from the open mattress areas. A big correlation was discovered between the every day variety of MRSA colonized or contaminated sufferers within the Unit and the every day variety of MRSA optimistic air samples cultures obtained (r2=0.128; P<0.005). The frequency of optimistic cultures was considerably larger within the single rooms than within the open mattress areas (relative threat=3.2; P<0.001). The outcomes from one of many single rooms confirmed a robust correlation between the presence of MRSA sufferers and MRSA optimistic air samples (relative threat=11.4; P<0.005). Our findings show that the presence of airborne MRSA in our unit is strongly associated to the presence and variety of MRSA colonized or contaminated sufferers within the Unit.
Affect of mattress making on a great deal of airborne and surface-associated drug-resistant micro organism in affected person rooms” (2023):
A transient improve in MRSA in room air was detected in most samples 1 min and 15 min after mattress making…, Floor samples confirmed that MRSA… was remoted commonly within the affected person atmosphere. Correlation between airborne and floor pathogen hundreds after mattress making was demonstrated. The research outcomes point out the significance of carrying a face masks together with cautious dealing with strategies when making the beds of sufferers carrying multi-drug-resistant micro organism. If the provider standing of a affected person is unknown, consideration must be given to protecting measures for employees and different sufferers current throughout and shortly after mattress making. Floor disinfection shouldn’t be began till at the least 30 min after mattress making.
Duh, you must let the micro organism settle earlier than you clear the surfaces! (In fact, MRSA is airborne in factory farms — however not, apparently, in hospitals!)
Now, it’s clear that fomite transmission is a pathway for MRSA transmission — virtually definitely the principle pathway, given profitable MRSA reductions previously. Nonetheless, except we’re prepared to simply accept a degree of continued MRSA transmission, it appears clear to me that airborne MRSA should be addressed, definitely on the degree of the precautionary rules. And if the HEPA filters arrange — one assumes — to entice SARS-CoV-2 additionally entice MRSA, is that so very dangerous? Or [dread word] the masks? (In fact, I’ve large priors on resistance to airborne, given the unconscionable and unscientific “huge resistance” to airborne transmission by WHO, CDC, and the Hospital An infection Management group. One other method of claiming that’s that these establishments have kind. And never good kind. Or accountability.)
Thankfully, the FDA has authorized a masks that blocks MRSA. So now let’s flip to present precautions to forestall MRSA.
Do Enhanced Barrier Precautions Handle Airborne MRSA Transmission?
We should match Enhanced Barrier Precautions (EBP) throughout the bigger framework of An infection Management as understood by CDC. From “An infection Management Fundamentals“:
There are 2 tiers of really useful precautions to forestall the unfold of infections in healthcare settings:
Normal Precautions and Transmission-Primarily based Precautions.
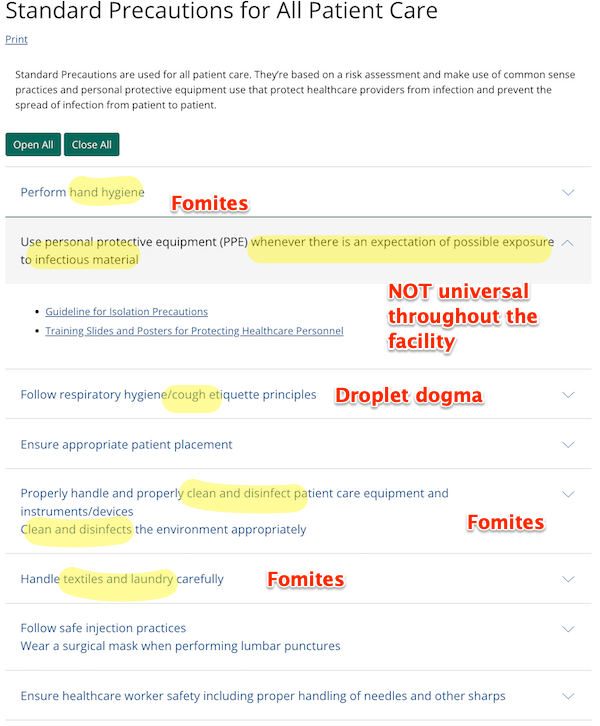
Normal Precautions (Web page final reviewed: January 26, 2016):
Normal Precautions are used for all affected person care. They’re based mostly on a threat evaluation and make use of frequent sense practices and private protecting gear use that shield healthcare suppliers from an infection and stop the unfold of an infection from affected person to affected person.
Extra particularly:
Transmission Precautions (Web page final reviewed: January 7, 2016):
Transmission-Primarily based Precautions are the second tier of fundamental an infection management and are for use along with Normal Precautions for sufferers who could also be contaminated or colonized with sure infectious brokers for which extra precautions are wanted to forestall an infection transmission.
Transmission Precautions at the least has an airborne part. Right here it’s:
![]()
Clearly these “precautions” are wholly insufficient to forestall transmission of an airborne, asymptomatic Stage 3 Biohazard (SARS-CoV-2) that strikes like smoke by means of the complete facility. I’m undecided they’re sufficient for MRSA both; that MRSA rose by 41% in the course of the early phases of the Covid pandemic would argue no. (Isn’t it superb how these “Precautions” don’t take account of the Precautionary Precept?)
And now we arrive at “Enhanced Barrier Precautions”, that are a 3rd tier of Precautions for Andrew “Ratface Andy” Cuomo’s demise traps nursing properties solely. From the CDC’s FAQ:
What are Enhanced Barrier Precautions?
Enhanced Barrier Precautions are an an infection management intervention designed to cut back transmission of multidrug-resistant organisms (MDROs) in nursing properties. Enhanced Barrier Precautions contain robe and glove use throughout high-contact resident care actions for residents recognized to be colonized or contaminated with a MDRO in addition to these at elevated threat of MDRO acquisition (e.g., residents with wounds or indwelling medical units).
What are the variations between Enhanced Barrier Precautions and Normal Precautions?
As a part of Normal Precautions, which apply to the care of all residents, using PPE relies on the “anticipated publicity” to blood, physique fluids, secretions, or excretions. For instance, gloves are really useful when contact with blood or different doubtlessly infectious supplies, mucous membranes, non-intact pores and skin, or contaminated gear may happen. A robe is really useful to guard pores and skin and stop soiling of clothes throughout procedures and actions that would trigger contact with blood, physique fluids, secretions, or excretions.
Enhanced Barrier Precautions develop using robe and gloves past anticipated blood and physique fluid exposures. They concentrate on use of robe and gloves throughout high-contact resident care actions which were demonstrated to lead to switch of MDROs to fingers and clothes of healthcare personnel, even when blood and physique fluid publicity just isn’t anticipated. Enhanced Barrier Precautions are really useful for residents recognized to be colonized or contaminated with a MDRO in addition to these at elevated threat of MDRO acquisition (e.g., residents with wounds or indwelling medical units). Normal Precautions nonetheless apply whereas utilizing Enhanced Barrier Precautions. For instance, if splashes and sprays are anticipated in the course of the high-contact care exercise, face safety must be used along with the robe and gloves.
See something about airborne there? Masks? Thought not. Kevin Kavanaugh as soon as extra:
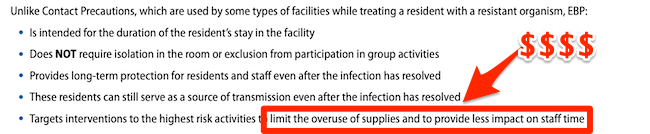
EBP permits contact precautions solely for use a few of the time, and the resident is allowed to roam across the facility. “Residents are usually not restricted to their rooms and don’t require placement in a non-public room.” Even with low transmission threat actions, resembling passing medicines, these actions are carried out so often that transmission can nonetheless happen.
Enhanced barrier precautions and never advocating for admission screening of main pathogens is the other of figuring out and modifying a affected person’s microbiome to forestall unfold to different people.
As soon as once more, there is no such thing as a idea that no matter is airborne can — definitely with SARS-CoV-2, probably with MRSA — unfold all through the ability.
Conclusion
Why then, provided that airborne tranmission is an enormous loophole for all CDC’s tiers of precaution, are Enhanced Barrier Precautions even being adopted by well being (putatively) amenities? The letter saying CDC’s new EBP steerage gives a clue:
Cash (musical interlude). Precisely as with CDC’s steerage on college air flow, as I present right here. So if someone in your care is in a nursing dwelling and will get MRSA, keep in mind that CDC didn’t shield them from airborne tranmission, and why.
NOTES
[1] Abaluck et al., the place a pure experiment permitted a randomized trial just isn’t listed, oddly. Or not.

[ad_2]
Source link










:max_bytes(150000):strip_icc()/Health-GettyImages-1477523726-d9489f5e044241b097588b0636bf7561.jpg "Solar Poisoning: Indicators and Signs")



















{kind=link}